
In case you missed it, Borgen, the well-received Danish political drama, is now streaming on Netflix. Think The West Wing but with more political parties and more Denmark. Highly recommended.
A prototype for a paper construction that’s been rambling around my head for the last couple of days. Inspired by Oliver, who had us listen to a meditation about “moving beyond grief” on the ferry sailing home on Monday, which got me thinking about focusing backward versus focusing forward.
The swooshing sound, which was accidental, is perhaps my favourite part of the mockup.
Kathleen Edwards, live from Stittsville, released her album Total Freedom in August.
She’s a big deal. And yet it seems like we used to hang out.
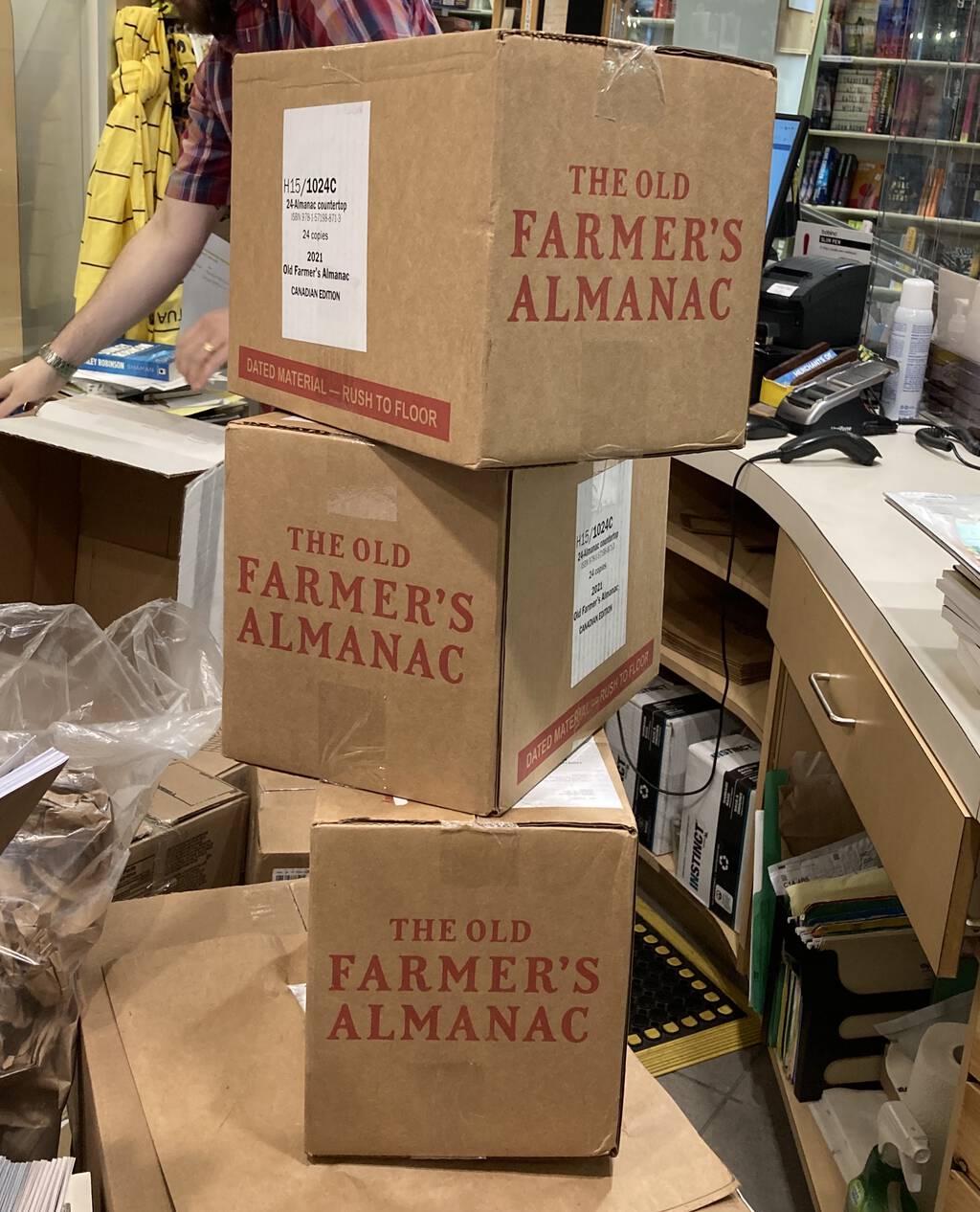
Three boxes of the 2021 edition of The Old Farmer’s Almanac landed at The Bookmark in Charlottetown today, and I encourage you to stop by and pick up your copy while there are still copies available.
When you buy The Old Farmer’s Almanac, not only are you getting a companion that’s “useful with a pleasant degree of humour,” but you’re also helping put food on the table of we at 100 Prince Street, as I enter my 25th year helping to maintain Almanac.com.
As a special bonus this year, you’ll also find an article by Charlottetown author (and my longtime friend) Ann Thurlow in the Canadian edition, so you’re really helping keep food in the pots of two Island households.
(Those of you from away are also encouraged to buy the 2021 edition: find retailers here).
The PEI Museum and Heritage Foundation has a podcast, the hidden island. There’s nary a fiddle nor old-timer-with-railway-story to behold.
Matt Webb writes about seizing the remote work hill:
So an ice cream van that pulls up, jingling out the MIDI version of Josh Wink’s Higher State of Consciousness at 11am, everyone on the street downing tools and heading out for a caffeine hit and to catch up with friends?
My workplace has not changed at all due the pandemic—it’s still just me and the machines in our underground church bunker—but I would welcome the chance to punctuate my day like this with all the other hidden toilers. As it stands, most days I don’t lay non-Zoom eyes on a single soul.
Postscript: Jeff Douglas (yes, That Jeff Douglas), once had a Piaggio Ape set up as a mobile espresso shop in Toronto; Machine Mobile gave up the ghost in 2018. That would have been perfect for this remit.
Oliver and I are on our last night of a week’s vacation on the eastern shore of Cape Breton Island; against traditon, I’ve maintained radio silence throughout, so as to perfect the art of doing absolutely nothing, which is a practice I do not come by honestly.
We have largely succeeded at carrying out a week of nothing but sleeping, eating, reading, sketching, watching TV, and going for walks on the beach, punctuated by a trip into Port Hawkesbury for supplies, and a run up to Judique for lunch.
Otherwise, save a lovely afternoon hosting my old friend George on Friday afternoon, we’ve been in pleasant isolation, enjoying good weather, fresh blackberries every morning, and the occasional game of Crazy 8s.
The closest vacation I’ve ever had to this one was the week that Catherine and I spent on the shore of Lake Superior in 1992 at a remote cabin; there was more nudity on that trip, but otherwise it was similarly “let’s try to do nothing for a week.” There’s a lot to recommend it, especially when the hearty mélange that is daily life includes an awful lot of not doing nothing for both me and for Oliver.
As I write our car is up the road charging at the garage of the owner of the house where we’re staying, we’re just back from our last walk on the rocky shore, and I’m plotting how to turn the remaining food in the fridge into a last supper (what can you make from carrots, naan, heavy cream, blueberries, honey and barbecue sauce?). Tomorrow we’ll make our way to Antigonish for lunch and an EV top-up, and we’ll then catch the 4:00 p.m. ferry to Wood Islands and home.
Oliver starts a new course at the University of PEI on Tuesday–Susan Brown’s Cool Britannia–and I have my first committee meeting of the fall season on Wednesday. It’s been good to have a break.


Charlottetown’s annual outdoor art festival, Art in the Open, sputtered to life yesterday for its 10th anniversary. Between the pandemic and the threatening (and then actual) rain, people were much fewer and far between, and much of the joie de vivre was bleached out of the event, exposing more starkly what we’d known all along: it’s as much about experiencing art in community as it is about the art itself. Without the community, it was a lonely, damp evening.
Although the annual Crow Parade was covided out of the festival, participants were encouraged to continue to casually dress up as crows; Oliver was one of the few to step up, reprising his costume from 2019, and adding a bovine element (hence “coo” rather than “caw”) as an homage to Russell Louder:
Despite the scant crows, the damp, and the sparse participation, there were highlights.
Norma Jean Maclean’s Work, in the oval at Confederation Landing Park, “a performance about day-to-day physical acts, searching for meaning in the mundane, and ultimately the processes of doing and undoing” was inspired.
Detail from “Work” by Norma Jean Maclean, August 29, 2020
Nine Yards’s Alone Together was intended as an installation, but was just as interesting as a performance piece, as we ambled along as it was being last-minute assembled (we returned later in the night and were able to walk inside and feel it pulse and rumble):
Detail from “Alone Together” by Nine Yards, August 29, 2020

Detail from “Alone Together” by Nine Yards, August 29, 2020
Hannah Bridger’s Wind Farm, on the great lawn in Victoria Park, was an interesting rumination on the wind:

“Wind Farm” by Hannah Bridger, August 29, 2020
I have long-admired Sandi Hartling’s work, and her anything at all, in the windows at the Confederation Centre Art Gallery entrance, was playful, especially in that (reflective) setting:

Detail from “anything at all,” Sandi Hartling, Confederation Centre of the Arts
By 6:30 p.m. the rain had begun in earnest and we’d done the waterfront-downtown-park loop. We ordered a pizza, paid one more visit to Nine Yards, and headed toward home.
On the way there we passed evidence of Becka Viau’s Revolution, wherein she rolled a round hay bale about the city. It was perhaps the piece that best summed up the contemporary zeitgeist.

Detail from “Revolution” by Becka Viau, August 29, 2020
We picked up the pizza and sought shelter at home for our regular Saturday Movie Night; Oliver insisted we watch a movie with an artistic theme, so we settled on The Best Offer.
I’m used to returning home from Art in the Open with a feeling for the endless possibility of the human endeavour; that feeling escaped me yesterday, replaced with a more basic satisfaction that art can perservere even in fraught times.
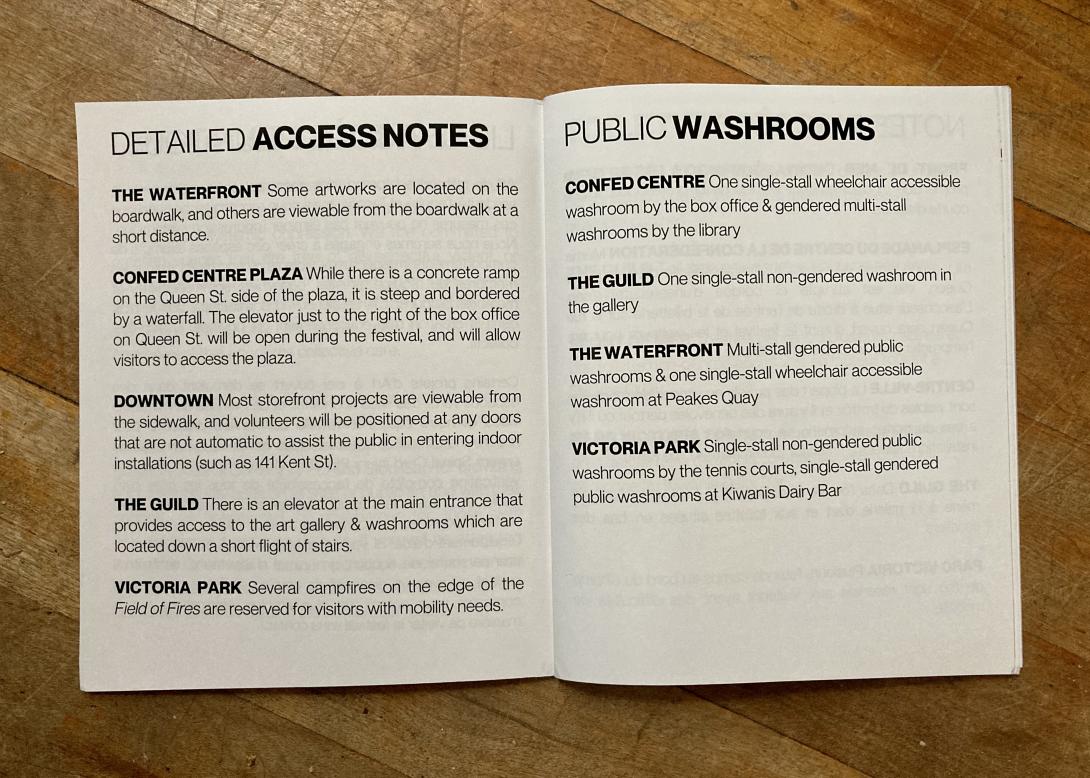
Kudos to Art in the Open for seeking to become accessible to all.
It was a hard cycle to the this morning: Oliver was grumpy, the trail was crowded, and we were both out of shape and overdressed for the weather.
But we persevered, made it to Gallant’s for our smoked salmon bagel, and then back down to the farmers’ market; once we had food and drink in us, brighter times prevailed.
If you’d told me a year ago that Oliver and I would successfully build a 12 km cycle into our Saturday morning routine I’d not have believed you. But I’m so glad we did: grumpiness notwithstanding, it’s the highlight of my week.
How does an overturned safe end up in the ditch beside the Confederation Trail? Oliver speculated it was a drunken burglary gone wrong. If you’re missing your safe, it’s between Joe Ghiz Park and the 1911 Jail.

About This Blog
 I am Peter Rukavina and this is my blog. I am a writer, letterpress printer, and a curious person.
I am Peter Rukavina and this is my blog. I am a writer, letterpress printer, and a curious person.
To learn more about me, read my /now, look at my bio, listen to audio I’ve posted, read presentations and speeches I’ve written, see things I’ve favourited elsewhere, or get in touch (peter@rukavina.net is the quickest way).
I have been writing here since May 1999: you can explore the 25+ years of blog posts in the archive.
![]() You can subscribe to an RSS feed of posts, an RSS feed of comments, an RSS feed of favourites elsewhere, or a podcast RSS feed that just contains audio posts. You can also receive a daily digests of posts by email. I also publish an OPML blogroll.
You can subscribe to an RSS feed of posts, an RSS feed of comments, an RSS feed of favourites elsewhere, or a podcast RSS feed that just contains audio posts. You can also receive a daily digests of posts by email. I also publish an OPML blogroll.
Instagram • YouTube • Vimeo • ORCID • OpenStreetMap • Internet Archive • PEI.art • Drupal • Github.