
I didn’t set off knowing what I was going to create last week, but it ended up as something of a visual expression of what grief feels like.
I started off with the words “I’m okay” in my head, evolving this into the all-caps I’M OK.
I set this in 120 point Akzidenz Grotesk, using a comma for an apostrophe:

I sliced up some letter-sized Staples house-brand 67 lb. card stock into cards 5½ by 4¼ inches in size to print on, just large enough, give or take, to qualify as a postcard for mailing.
Since seeing a printer mix inks with a palette knife the other day, I’d been eager to try this out for myself, and so I started with white and added just the faintest touch of yellow
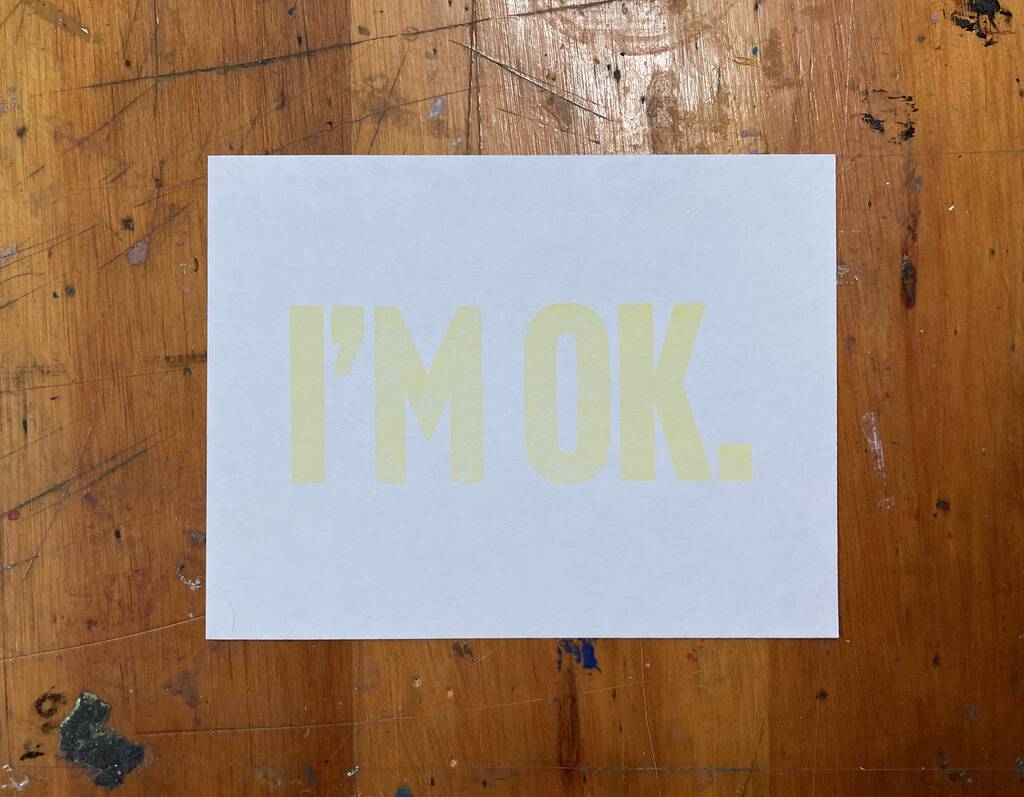
Seeing that I’M OK hovering on the card, barely visible in some lights, I was struck suddenly with the feeling that a very tentative sense of “I’m okay” was something I’ve felt frequently over recent months. But it’s not always tentative: sometimes it’s very strong. And sometimes it’s halfway in the middle.
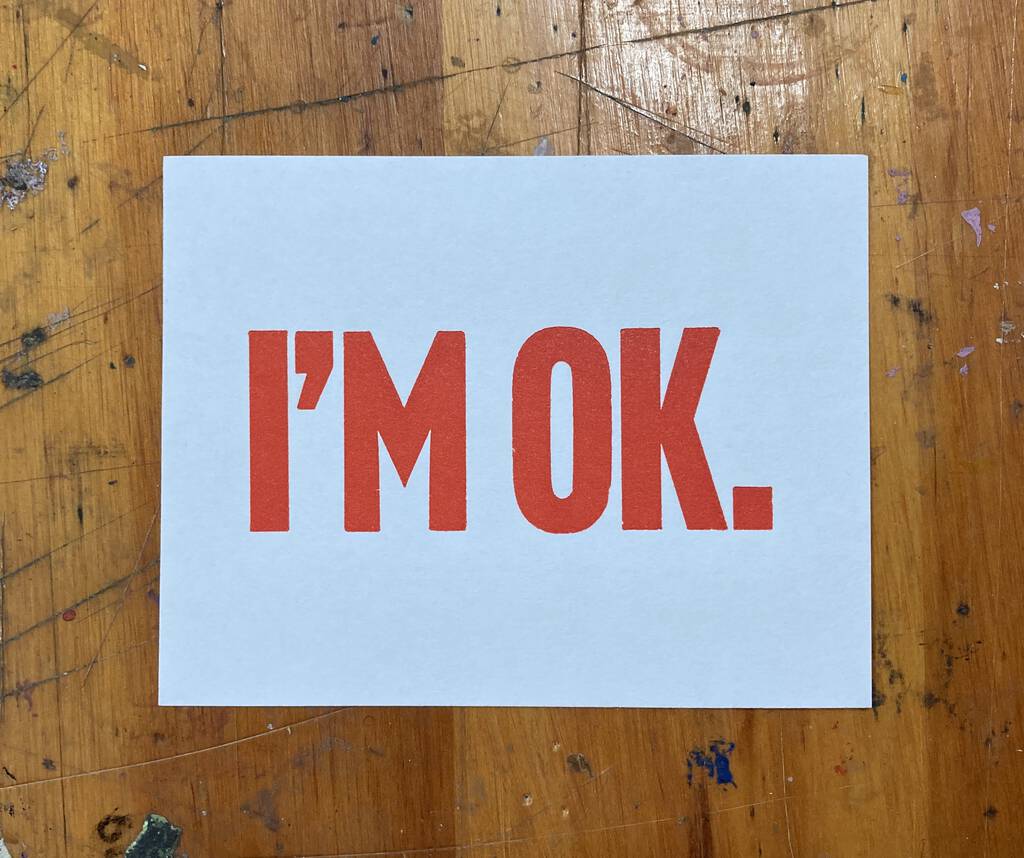
So I added a little more yellow, and printed some more obviously-yellow cards. And then added some red to get some orange cards. And then even more red to get what amounts to a bold declaration, more an “I’m okay!” than an “I’m okay.”
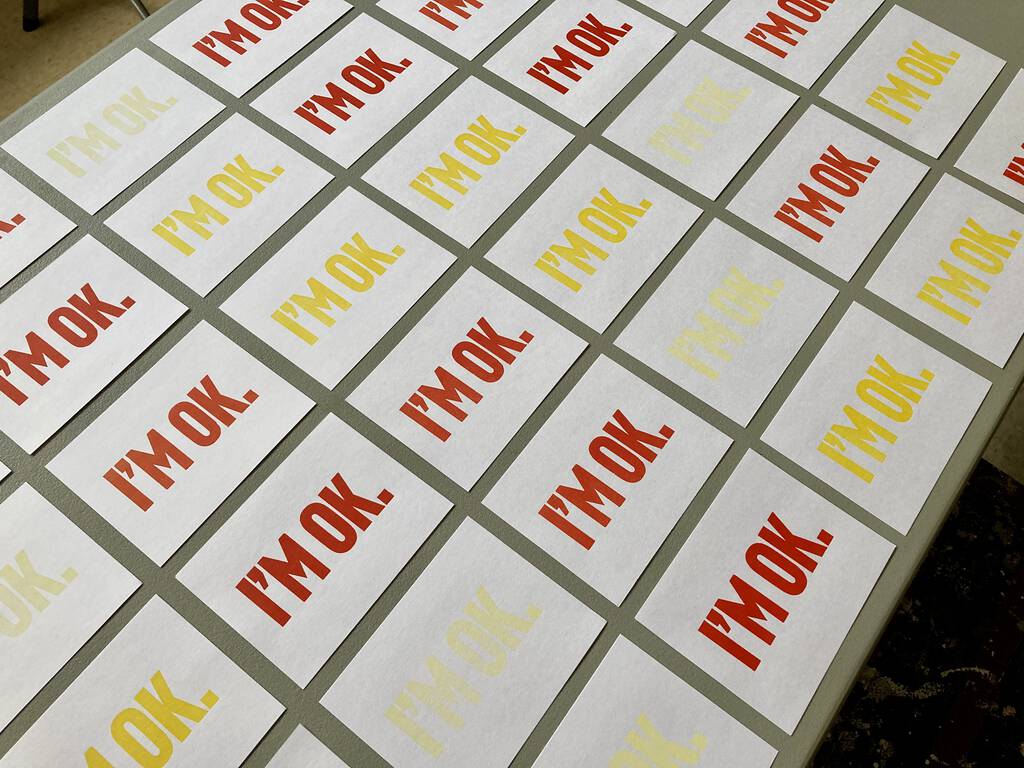
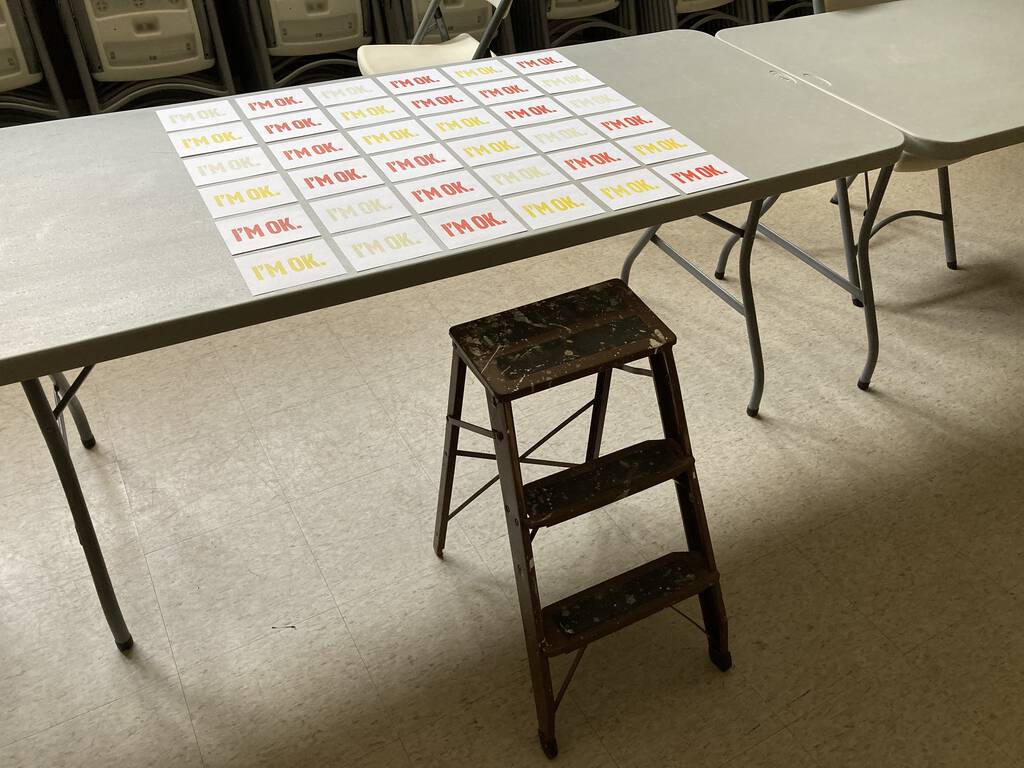
Put together in a montage, these various shades of being okay ended up becoming something even more familiar, the ebb and flow of being okay, and not being okay, and being very okay, and then shudderingly not being okay at all. That is what grief feels like. And I accidentally found a way to express it typographically.
I first reported on the number of electric vehicles registered by the Province of PEI last year; I received updated numbers for 2020 late last week, and here’s a year-on-year comparison:
| Vehicle Type | 2019 | 2020 | Increase |
|---|---|---|---|
| Battery Electric | 33 | 84 | 150% |
| Hybrid | 403 | 862 | 113% |
| Plug-in Hybrid | 7 | 57 | 714% |
| TOTAL | 443 | 1,003 | 126% |
“Battery electric” vehicles are ones that run entirely on electricity; “hybrid” vehicles run on both gasoline and electricity but don’t plug in (the battery is charged by the gasoline engine), and ”plug-in hybrid” vehicles run on both gasoline and electricity (and the battery is charged both by the gasoline engine, and if plugged into the mains).
I suspect that the dramatic more-than-doubling in electric vehicles over the last year is due a combination of an actual increase and in better data quality control, spurred by the fact that electric vehicles are entitled to free motor vehicle registration. Nonetheless, the growth is good to see.
This past weekend was the 2020 edition of the Cloggeroo folk festival in Georgetown, an event that Oliver’s attended almost since it was founded; indeed, it was among his first nights away from home without us when he spent the Cloggeroo weekend camping with Derrick in 2015.
Except that this weekend wasn’t the 2020 edition of Cloggeroo, as, due COVID-19, Cloggeroo was cancelled this year.
This cancellation wasn’t enough to deflate Oliver, however: he insisted we carry on with the standard Cloggeroo operating template, without the folk music parts. He did this with his typical deft crafting of a series of suggestions that ultimately led me to arrange this without his coming right out and stating his case.
And so I booked us two nights at Deroma Waterfront Cottages in Georgetown Royalty, and our visit east coincided with the start and end of the non-Cloggeroo.
I’d been part of the Cloggeroo weekend myself before: in 2017, absent other support, I was Oliver’s assistant photographer, but we returned to town every night that year, and I’d never had the full-on nights-on-the-Brudenell experience.
Deroma turns out to be an entirely pleasant riverside cottage resort with the kinds of cottages that you might remember from childhood vacations in the 1970s: not architectural masterpieces, but solidly-built, spotlessly clean, well-equipped cottages generously spaced over a nicely treed lot. There was a badminton court, a volleyball court, a basketball court, kayaks for the borrowing, fire pits on the beach, and warm(ish) water to swim in.

Without The Rubber Boot Band to entertain us, we made our own fun.
On Friday night we grilled (veggie) burgers on the barbecue on the deck (which I managed to do without blowing the place up; fire-affairs was always Catherine’s department), went for a walk on the beach, and the went into Georgetown to do our regular Family Zoom from the beach in Georgetown (thus achieving a kind of Cloggeroo-simulacrum).
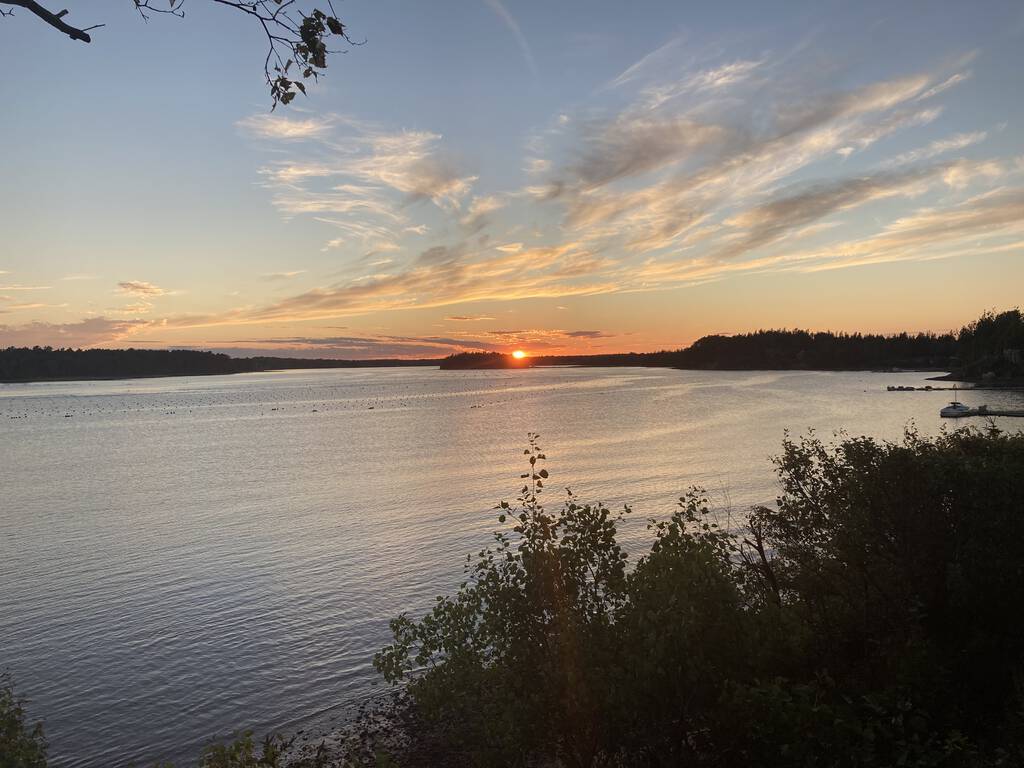
On Saturday we had smoked salmon bagels for breakfast (some habits cannot be broken, no matter the location), went in search of Poxy Island (yes, there is an island called Poxy Island, named because it was a place for smallpox quarantine; we failed in making our way there, but did have an angry owner of a highfalutin cottage shake his fist at us for trying), walked up the road to visit our friend Ray (and then walked back down to the cottage along the shore at low tide), made an attempt to participate in Pen Night despite the very shaky wifi, and enjoyed a spectacular sunset back at Ray’s afterwards.
Sunday morning we woke up, had (store-bought) waffles for breakfast, packed up our gear, and checked out, happy to have had a short break from town. We stopped to top-up the EV in Montague, had tacos at the newly-opened Totally Taco for lunch, and were home mid-afternoon.
Postscript: Oliver prepared four Spotify playlists to go with each of the days:
These playlists correspond to what would have been the four chunks of Cloggeroo, had it happened.
There is much to love about Mandy Patinkin’s YouTube channel, including considering the prospect of Mandy and his wife Kathryn Grody living in an RV for six weeks.
Many years ago, Catherine and I, and our friends Lisa and Stephen, set off from Charlottetown to drive Stephen to the train home to Ontario.
For reasons of whimsy, we opted to drop Stephen at a flag stop in northern Maine; for reasons of lateness we split the trip in two, camping just the other side of Moncton halfway.
These were the days when Catherine was a serious coffee drinker and I was not a coffee drinker at all, and so when we woke up the next morning it was vital for Catherine to get coffee in a way I didn’t understand at all. At my assholish insistence, we drove all the way to Saint John—about 90 minutes—before coffee was secured. It was almost the death of us.
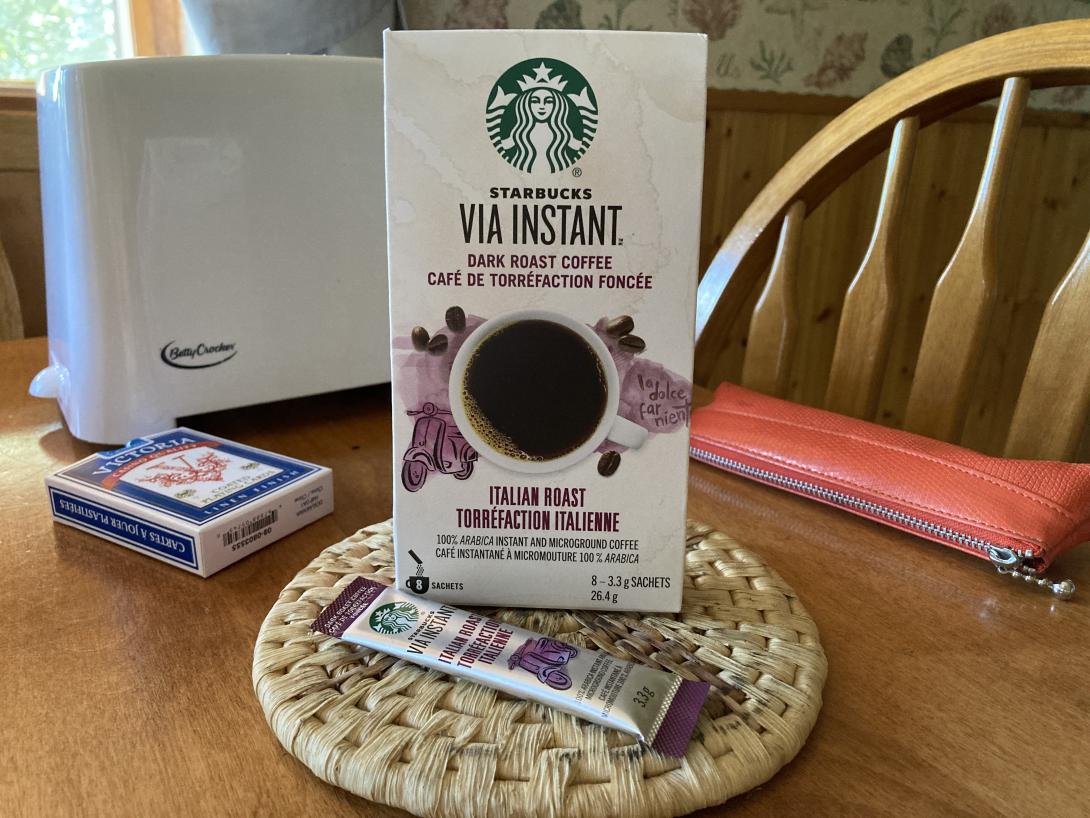
Now that I am a serious coffee drinker myself, in retrospect I take Catherine’s side of that divide. And so I was sure to acquire coffee to take with us for our weekend cottage stay in Georgetown Royalty.
Starbucks “Via Instant” turns out to be significantly more than palatable instant coffee, leaps and bounds better than the instant of yore. Boil water, add packet of “microground” coffee, stir, drink.
If only such innovations existed in the mid-1990s.
Oliver and I went over to Memorial Hall at Confederation Centre of the Arts for the Artist Trading Card event last night.
The setup was similar to previous years, but for the palpable feel of COVID in the air. Oliver, ever receptive to any hint of tension coursing through the zeitgeist, was somewhat on edge, to the point where minor violations of (his) protocol, like only my name being written on the Ziploc bag provided for card-collecting, came close to sending him over the edge. But we made our way, and things simmered to a low, sustainable boil.
There were 40ish participants, each of us bringing 39ish cards, so that we all left with one of everything. My entry was unique inasmuch as there were four parts to it: WE, ARE, HERE, plus a loose-leaf binder ring. I put an example of the ring-grappled cards at the head of the table as a guide, but otherwise left it to people to figure out what to do (leaving one of the most interesting aspects of the night, for me, eavesdropping on conversations among the others: “what, um, are we supposed to, um, take all three?”). Because I put 40 of each card, and 40 rings, out on the table, at the end of the night I had analytics to show that 5 people took only a WE, unable to take the hint (and/or perhaps having nobody to whisper to for support).
It would be a stretch to call the evening “fun,” given the heat, the noise, the mask-wearing, the aforementioned tension. But I’m glad I did it nonetheless, and I’m glad Oliver came with me.
Every weekday morning for three years I drove Oliver to Colonel Gray Senior High School. When we arrived at the school, I would text his educational assistant–usually Dave, but sometimes Jill or Laura or Maritza—so that they’d know to come outside and fetch him to go on their morning constitutional.
We are here, I texted every morning like clockwork:
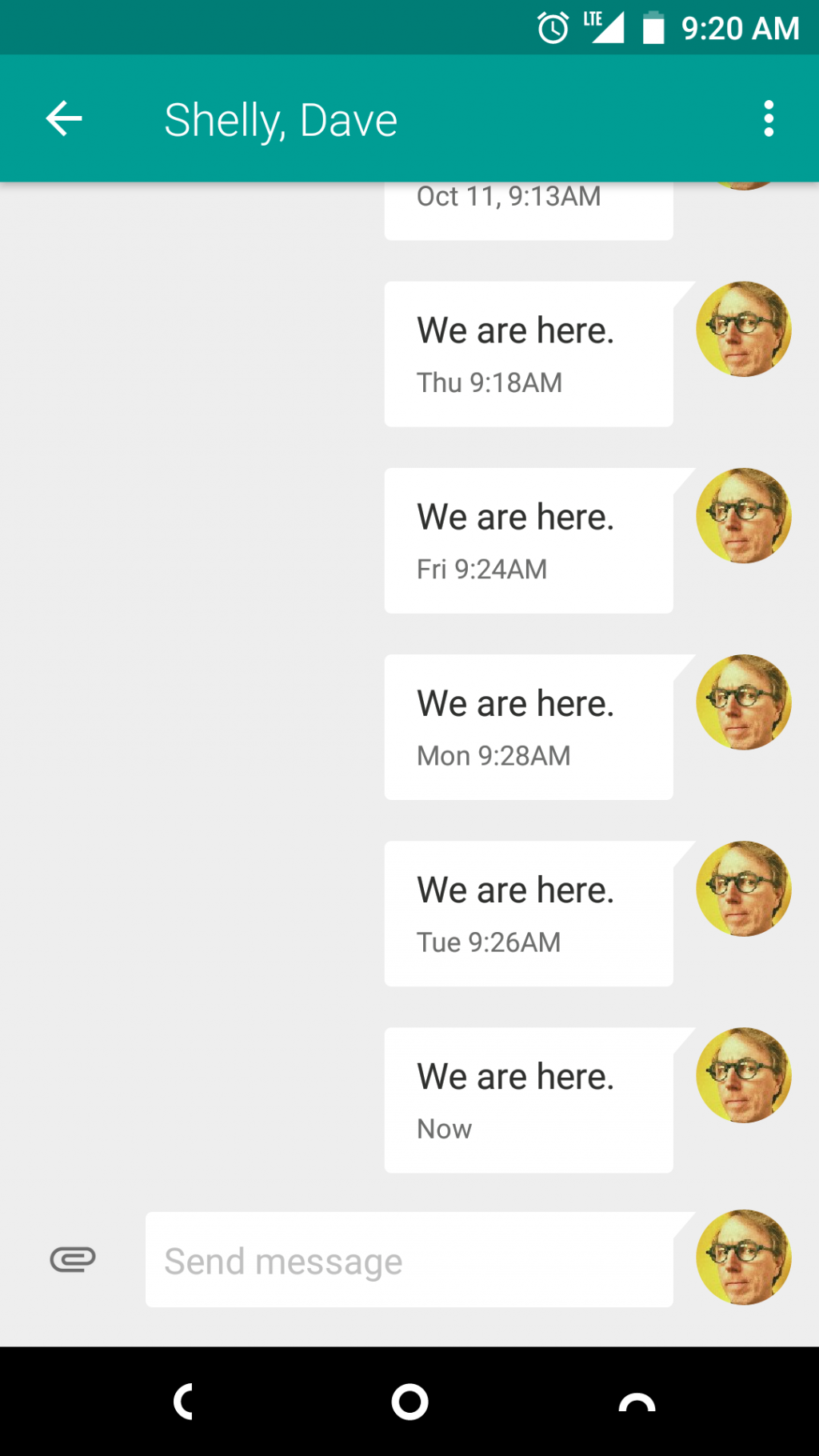
Oliver turned this into a stirring recitation one morning when we had a little bit of extra time to kill in the car while waiting.
When it came time to pick a subject for tonight’s Artist Trading Cards event at the Confederation Centre of the Arts, We Are Here popped into my mind as a kind of baseline statement of claim for humanity.
The times may be challenging, but we are here. So to speak.
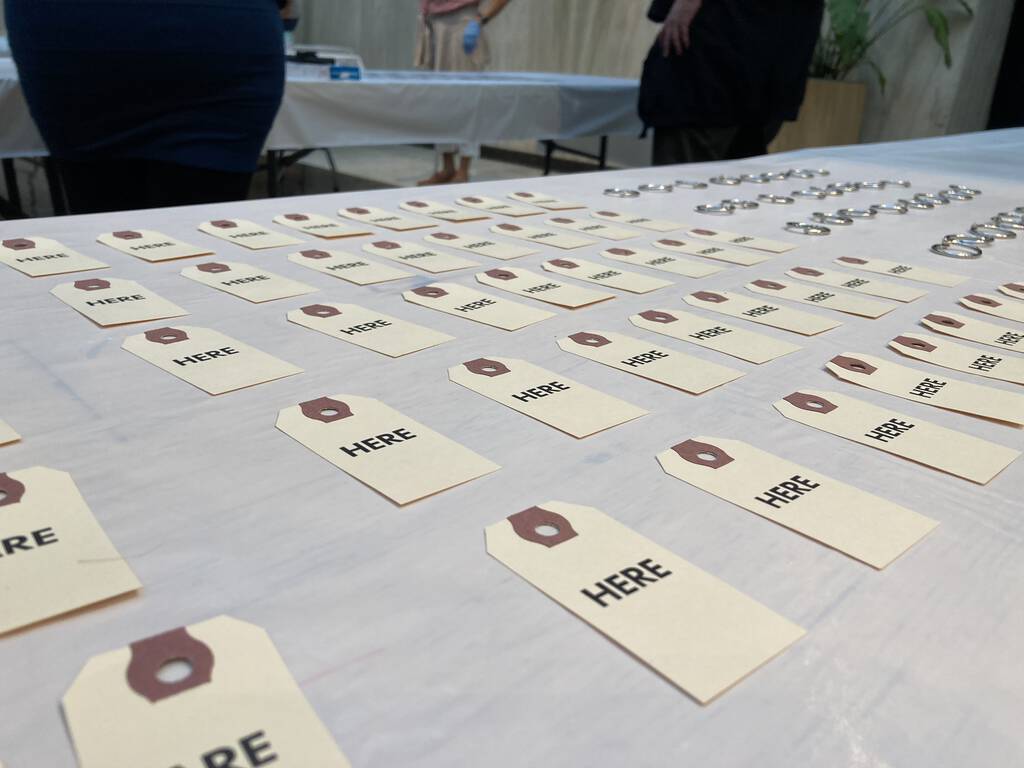
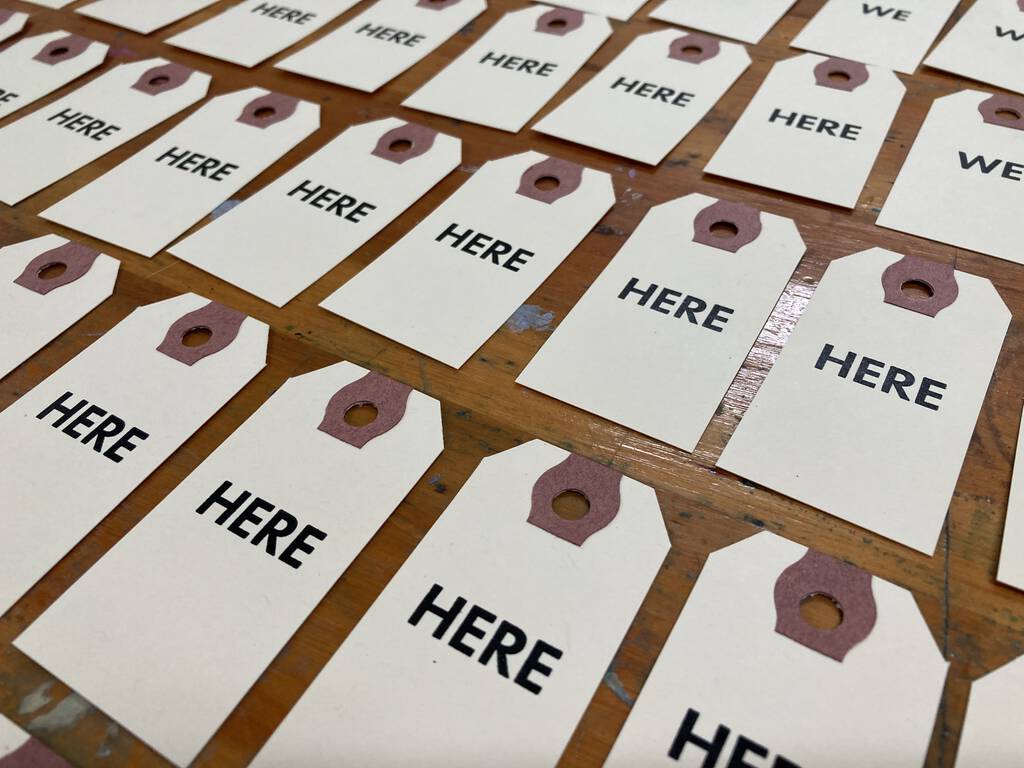
I had a couple of 100 packs of № 1 shipping tags here in the shop, and decided to use those as a starting point (shipping tags come in standard sizes; № 1 are the smallest, at 70 mm by 35 mm).
I chose 30 point Futura Bold (acquired in 2015 from Letterpress Things) for the typeface, and Southern Ink Dense Black as the ink. I experimented with using upper and lower case, but opted for all caps for symmetry’s sake.
Shipping tags turn out to be a joy to print on: they’re nice and meaty, easy to get in and out of the press, quick to dry.
I printed 50 each of WE, ARE and HERE:

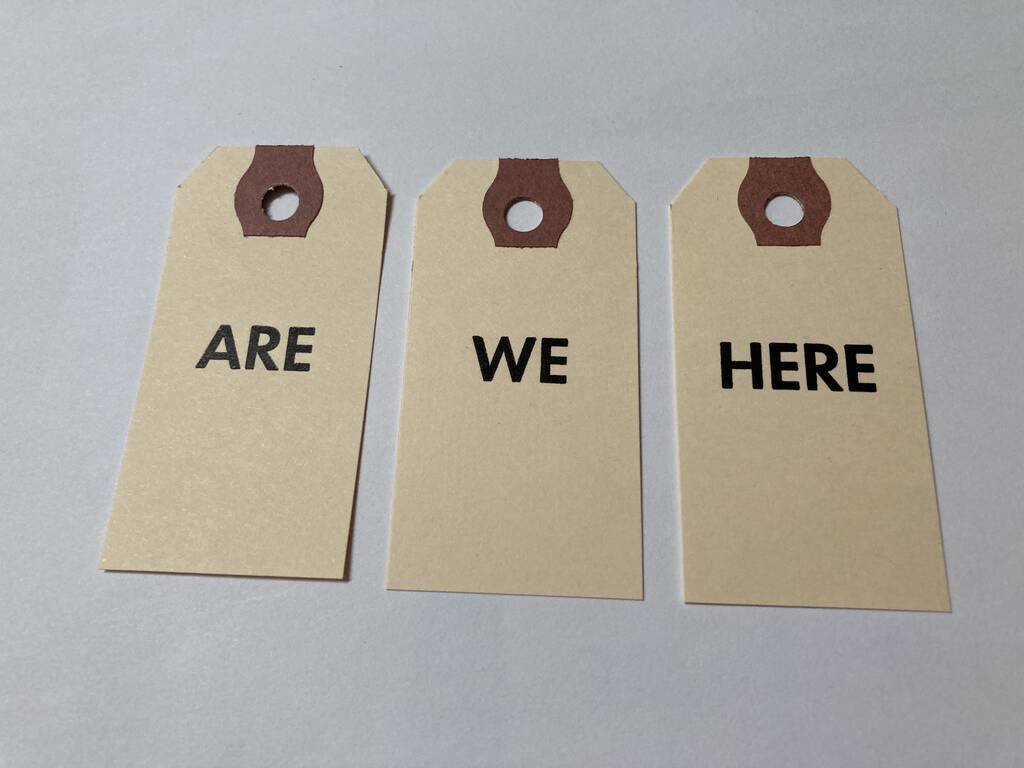
Once they were printed and dried, I decided that my artist trading card partners would need something to lasso their sets together, so I purchased three boxes of 1 inch silver “loose leaf rings” from Staples:

While I went into this project thinking WE ARE HERE, I realized, as I continued, that there are many combinations that can be made from these three words:
WE ARE HERE
WE HERE ARE
ARE WE HERE
ARE HERE WE
HERE WE ARE
HERE ARE WE
Mathematically, to calculate the number of permutations in this case, where there are 3 objects combined into sets of 3, you simply add up the integers from 1 to 3, so 1 + 2 + 3, to get 6 possible combinations.
I’ll be trading sets tonight at the Confederation Centre of the Arts, starting at 7:00 p.m. Unfortunately, due COVID, it’s not a public event, so you’ll have to use your imagination to recreate the thrill of the trade.
My font of 120 point Akzidenz Grotesk is missing the apostrophe. But there’s a comma. And what is a comma but an apostrophe in need of a lift.

Spotted near the Murphy Community Centre on Richmond Street in Charlottetown: “No Parking” has given way to the “circle P slash.”

About This Blog
 I am Peter Rukavina and this is my blog. I am a writer, letterpress printer, and a curious person.
I am Peter Rukavina and this is my blog. I am a writer, letterpress printer, and a curious person.
To learn more about me, read my /now, look at my bio, listen to audio I’ve posted, read presentations and speeches I’ve written, see things I’ve favourited elsewhere, or get in touch (peter@rukavina.net is the quickest way).
I have been writing here since May 1999: you can explore the 25+ years of blog posts in the archive.
![]() You can subscribe to an RSS feed of posts, an RSS feed of comments, an RSS feed of favourites elsewhere, or a podcast RSS feed that just contains audio posts. You can also receive a daily digests of posts by email. I also publish an OPML blogroll.
You can subscribe to an RSS feed of posts, an RSS feed of comments, an RSS feed of favourites elsewhere, or a podcast RSS feed that just contains audio posts. You can also receive a daily digests of posts by email. I also publish an OPML blogroll.
Instagram • YouTube • Vimeo • ORCID • OpenStreetMap • Internet Archive • PEI.art • Drupal • Github.